
Narrowing of the Spinal Canal

Spinal Canal Narrowing Home Page / Spinal Canal Narrowing (Lumbar Spinal Stenosis) The spinal canal is the canal through which the spinal cord and nerves exiting the spinal cord travel within the vertebrae. Numbness and hardening of the soft tissue and bone structures that form the spinal canal can occur as a result of various factors, including trauma, abuse, and genetic factors. This narrowing can occur in this canal. This results in nerve root compression. These patients complain of pain and numbness in the calf, particularly when standing for long periods and walking. The pain is relieved or relieved when sitting and bending forward. Symptoms: Leg pain worsening with standing and walking; Numbness and tingling in the calves; Relief with sitting and bending forward; Neurogenic claudication (pain worsening with walking); Feelings of weakness in the legs. Treatment: Surgical Treatment: In this treatment, the spinal canal stenosis is opened (laminectomy and foraminotomy) to release the compressed nerves and spinal cord. Sometimes, the vertebrae are fixed with screws (platinum) to prevent misalignment. RELATED DISEASES: Lumbar Spondylolisthesis, Hydrocephalus, Spinal Cord Tumors
Lumbar Spondylolisthesis

Lumbar Spondylolisthesis Home Page / Lumbar Spondylolisthesis (Spondylolisthesis) is the forward slippage or displacement of two adjacent vertebrae, the upper vertebra relative to the lower vertebra. Symptoms: Low back and leg pain; Leg pain that worsens with walking and causes the patient to stop and collapse at a certain distance; Leg cramps; 1. Conservative Treatment: Restriction of certain movements; Analgesic-anti-inflammatory drugs; Local injections; Electrotherapy; Massage; Heat therapy; Exercise; Brace application. 2. Surgical Treatment: Surgical treatment may be necessary in the following cases: Patients with progressive neurological deficits (nerve weakness); Patients whose complaints persist despite medication and physical therapy; Patients with posture and gait disorders. Treatment Goals: To relieve low back and leg pain, prevent the progression of the spondylolisthesis, stabilize the unstable (mobile) segment, and improve posture and balance. In surgical treatment, compressed nerves are released, and the vertebrae affected by the spondylolisthesis are fixed with screws (platinum). RELATED DISEASES: Hydrocephalus; Spinal Cord Tumors; Brain Hemorrhages
Hydrocephalus
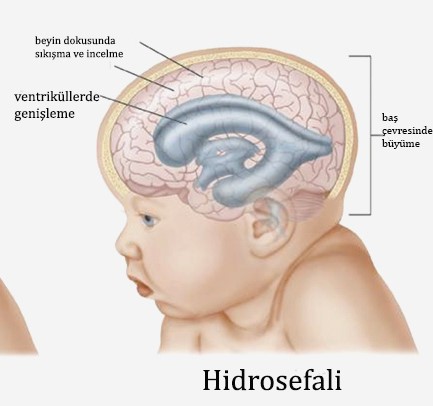
Hydrocephalus (Water Accumulation in the Brain) Home / Hydrocephalus (Water Accumulation in the Brain) Hydrocephalus is a term derived from the words hydro = water and cephalus = head. It is generally known as excessive water accumulation in the brain. The water referred to here is "cerebrospinal fluid." An increase in the amount of this fluid, found in certain chambers of the brain, causes increased pressure within the head and can damage the brain. Cerebrospinal fluid is constantly produced and reabsorbed throughout the day. This fluid surrounds the brain and spinal cord and has a continuous circulation. It has three primary functions: to reduce the harmful effects of trauma to the brain and spinal cord, to help nourish the brain and transport waste, and to regulate changes in pressure within the brain by circulating between the brain and spinal cord. Hydrocephalus can occur at any age, but it most commonly occurs in children and the elderly (over 60). Approximately one in 500 children develops hydrocephalus. In most of these cases, diagnosis is made at birth, prenatally, or in early infancy. Although rare, it can be due to genetic (hereditary) disorders or developmental disorders. Common causes include intracerebral hemorrhages, head trauma, brain tumors, hemorrhages due to premature birth, and meningitis. Symptoms of hydrocephalus vary from person to person. Common symptoms are listed below by age group. In newborns (0-2 months) Excessive head growth Thinning of the scalp Prominence of veins in the head Vomiting, restlessness Downward turning of the eyes Seizures or inability to communicate In children (2 months and older) Abnormal head growth Headache, nausea, vomiting, fever Double vision, restlessness Regression in walking or speech Communication disorder Loss of sensory-motor functions, seizures Difficulty staying awake or staying awake Middle-aged adults Headache Difficulty waking or staying awake Balance disorder Urinary incontinence Personality disorder Dementia Vision disorder In the elderly Communication disorder Unsteadiness while walking Difficulty remembering Headache Urinary incontinence Diagnosis In a patient with hydrocephalus, your doctor will talk to you, ask questions, examine you, and order some tests (Brain Tomography, Magnetic Resonance Imaging, Brain Ultrasonography) before starting treatment. The diagnosis of hydrocephalus, its cause, and what treatment process is required will be clear after these tests. A large head alone does not indicate hydrocephalus in children. However, the diagnosis is confirmed using brain imaging techniques. If the diagnosis is made in the womb before the baby is born, a report from the hospital ethics committee is required for pregnancy termination according to current laws. Causes of Hydrocephalus The causes of hydrocephalus vary by age group. 1- Newborns (0-2 months) Congenital: These patients constitute the largest group. Hydrocephalus may be present alone or in conjunction with other congenital anomalies of the spine (meningomyelocele). Intracerebral hemorrhages: Brain chambers often enlarge following spontaneous hemorrhages. 2- Children and adults Brain infections Brain hemorrhages Brain tumors Head trauma 3- The elderly Normal pressure hydrocephalus: Enlargement of the brain chambers following decreased absorption of cerebrospinal fluid. Hydrocephalus Treatment: Medication is not possible for hydrocephalus. Hydrocephalus can only be corrected through surgical interventions performed by neurosurgeons. The surgical procedures chosen will vary depending on the underlying cause of hydrocephalus. If there is an obstruction causing cerebrospinal fluid circulation, surgical treatment can be performed to address the cause (tumor, cyst, etc.). If the obstruction cannot be relieved, the intracerebrospinal fluid circulation pathways can be surgically altered. Because restoring cerebrospinal fluid circulation is not possible in most patients, the fluid must be diverted from the brain to another body cavity. This transfer involves a long, thin, elastic, silicone tube called a "shunt." A pump is located under the scalp to operate in one direction and at a controlled rate. Excess cerebrospinal fluid is transported to another part of the body through this thin tube, preventing increased pressure within the brain. However, because the brain constantly produces fluid, this system must operate continuously. Because the shunt is located under the skin, it can only be detected externally in infants. In children and adults, the tube can be felt under the skin. The shunt is surgically placed under general anesthesia. A small hole is drilled in the skull, and the end of the shunt is placed in the chamber within the brain that contains cerebrospinal fluid. A tunnel is then drilled under the skin of the head, neck, and abdomen, and the other end of the shunt is directed into the heart or abdominal cavity, where this fluid can be easily absorbed. Short-term antibiotics may be used to prevent postoperative infection. The patient is monitored in the hospital for a period after surgery. Symptoms usually improve after a while. However, if permanent damage has occurred to the brain tissue, some functions may not recover. The most important reason for failure to recover functions such as vision and intelligence is delayed treatment. The length of a patient's hospital stay varies depending on the patient's recovery. These patients require long-term monitoring to monitor the shunt's functioning. A significant portion of patients treated for hydrocephalus can lead normal lives. If the shunt fails or becomes infected, it may need to be replaced. In a third ventriculostomy, a hole is drilled in the skull using a camera-equipped endoscope to release adhesions within the brain cavities, thereby promoting the circulation of accumulated fluid. RELATED DISEASES Spinal Cord Tumors Brain Hemorrhages Brain Tumors
Spinal Cord Tumors

SPINAL CORD Tumors Home Page / SPINAL CORD TUMORS Spinal tumors are tumors located in the spinal cord and nerve roots within the spinal cord and spinal canal. These tumor cells continue to grow uncontrollably and cause harm to the patient. Spinal tumors can be benign (benign / non-cancerous) or malignant (malignant / cancerous). Primary tumors refer to tumors that originate in the spine or spinal cord itself, while metastatic tumors refer to tumors that have spread from elsewhere in the body to the spine. Spinal tumors can occur in three main areas: cervical (neck), thoracic (back), lumbar (lower back), and sacral (tailbone). They are also classified according to their location in the spine such as anterior (front) or posterior (back). Spinal tumors (spinal cord tumors) are associated with heavy morbidity and mortality rates (illness and death); It has become a focus of neurosurgery due to the positive outcomes achieved with early diagnosis and appropriate treatment methods. In parallel with technological advances, increased diagnostic capabilities and the development of surgical techniques, especially microsurgery, have increased treatment success rates. Approximately to of central nervous system tumors are located in the spinal cord. The prevalence of spinal tumors in the population varies between 2 and 10 per 100,000. Separating spinal tumors by location facilitates diagnosis and treatment. Therefore, the relationship with the dura mater (the outer layer of the spinal cord membrane) is taken into account in classification. Spinal tumors are classified accordingly as extradural, intradural extramedullary, and extramedullary. The ratio of intradural to extradural is 2:3. Of all spinal tumors, are extradural, are intradural extramedullary, and %5 are intradural intramedullary. Extradural tumors constitute the majority of tumors. In addition to metastatic tumors, primary spinal tumors are also included in extradural tumors. Neurofibroma and meningioma constitute the majority of intradural extramedullary spinal tumors. Ependymoma, astrocytoma, and hemangioblastoma constitute the majority of intradural intramedullary spinal tumors. Spinal tumors are predominantly benign. Improvements in early diagnosis and treatment have yielded better outcomes. Treatment primarily aims to remove the entire tumor (total), and most tumors are generally amenable to this treatment. General Clinical Findings and Diagnostic Methods: Both benign and malignant tumors present with pain in the back or lower back that is not related to movement. This pain is usually not caused by trauma, exercise, or stress. However, the pain increases with exercise and is more pronounced at night. Pain can spread to the hips, legs, or arms if the tumor is in the neck, and conservative treatment is not effective. While the patient's symptoms and complaints vary depending on the tumor's location, they generally occur when the tumor grows and presses on the spinal cord, nerve roots, or blood vessels. Compression of the spinal cord by itself is life-threatening. Additional symptoms include: Weakness or numbness in the arms and legs Difficulty walking, which can lead to falls Loss of pain and temperature sensation Impaired bowel and bladder control Paralysis can occur in varying degrees Scoliosis or other spinal deformities can result from large but benign tumors. DIAGNOSIS The first step in diagnosis begins with the patient's history and examination. A radiological diagnosis is performed to confirm this. A thorough neurological examination can help pinpoint the tumor's location. Plain X-ray: This x-ray reveals the bone structure. It is helpful only if the tumor has caused a bone lesion, but it is not possible to determine whether it is an infection or a tumor. Computed Tomography (CT) This imaging allows for diagnosis, measurement of canal diameters, and a clear view of bone structure. Magnetic Resonance Imaging (MRI) Using computer technology and magnetic resonance imaging, a three-dimensional image of the body can be created. Unlike other imaging techniques, MRI provides a highly accurate image of the nerve roots, spinal cord, surrounding soft tissue, and tumor. Once the tumor is identified, definitive determination of whether the tumor is benign or malignant can be made by taking a sample of the tumor and examining it under a microscope. If the tumor is malignant, pathology can also reveal its type. If the tumor is metastatic, a primary diagnosis should be made using abdominal ultrasound, CT scans, and similar tests. Treatment Options: Surgical Treatment. The primary goal is to surgically remove the entire tumor, and most tumors are generally amenable to this treatment. The indication for surgery depends on the type of tumor. Primary spinal tumors should be completely removed, if possible, to ensure a potential cure. The goal in metastatic tumors is to relieve the patient's pain, improve spinal stability, and treat or prevent neurological deterioration. Surgical treatment for metastases can be considered if the patient's life expectancy is longer than 12 weeks and the tumor is resistant to radiotherapy and chemotherapy. Other indications include pain that is resistant to medication, poor spinal stability, and compression of the spinal cord. Surgical Approaches: Posterior approach: The nerve roots and dura mater are exposed via the posterior approach. Anterior approach: Anteriorly located tumors are more easily controlled via the anterior approach. 360-degree approach: Both anterior and posterior approaches can be performed in the same session. CyberKnife Radiosurgery: Significant advances have been made in radiosurgery in recent years. CyberKnife radiosurgery has been beneficial in pain control and improving quality of life. Short treatment times, rapid recovery, and a positive response to treatment are considered the primary benefits of CyberKnife radiosurgery. This technique can be used primarily for spinal lesions, but can also be used in inoperable cases, in patients who have previously received radiotherapy, or as an adjunct to surgery. RELATED DISEASES: Lumbar Spondylolisthesis, Hydrocephalus, Cerebral Hemorrhage
Brain Hemorrhages
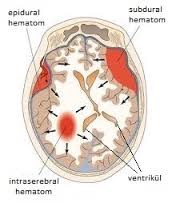
Brain Hemorrhages Home Page / Brain Hemorrhages A brain hemorrhage occurs when bleeding occurs within the brain due to the rupture of an artery within the brain. When a hemorrhage occurs, the brain, located within the skull, which is an inflexible structure, is subjected to pressure from the fluid filling it, crushing it, and various symptoms occur as a result. Types of Brain Hemorrhages Epidural: Between the skull and the dura mater, the outermost layer of the brain Subdural: Between the dura mater and the brain Subarachnoid: Between the meninges Intracerebral: Within the brain tissue Epidural Hematoma: A membrane called the dura mater covers the brain. The vessels above this membrane can bleed when broken or cracked skull bones cause injury. The resulting bleeding accumulates between the dura mater and the skull bones, compressing the brain. If surgery is not performed, brain death occurs, and the patient dies. Subdural Hematoma: Severe trauma can damage the vessels above the brain. Blood leaking from these vessels accumulates under the dura mater (brain membrane), causing further compression of the brain. Subarachnoid (Aneurysm/Blister) Hemorrhage: Bleeding can also occur beneath the arachnoid membrane, the very thin membrane covering the brain. These types of hemorrhages are caused by bubbles in the blood vessels called aneurysms. Intracerebral Hematoma: Bleeding into the brain tissue. It usually develops in patients with hypertension or due to a sudden increase in blood pressure. All these types of hemorrhage can occur in patients taking blood thinners (Coraspin, Plavix, Coumadin). Treatment: The goals of treatment are to save life, relieve symptoms, eliminate the cause of bleeding, and prevent the development of adverse events. Coma treatment can be summarized as placing the patient in the appropriate position, maintaining a patent airway, providing life support, and inserting a thin plastic tube into the fluid-filled areas of the head to reduce intracranial pressure. Surgical treatment is usually required. This craniotomy (OPEN) procedure involves opening the skull and draining blood from above or below the membrane, or from within the brain, depending on the type of bleeding. For aneurysm bleeding, a clip is placed on the aneurysm (open surgery) or an endovascular procedure is performed by sending a coil (spring) into the brain through one of the groin arteries. The type of surgery will be determined after an angiogram. Surgery may also be necessary to address large amounts of bleeding within the brain. RELATED DISEASES: Lumbar Disc Spondylolisthesis, Hydrocephalus, Spinal Cord Tumors
Brain Tumors
BRAIN TUMORS Home Page / Brain Tumors Brain tumors are tumors that form as a result of abnormal growth of normal cells in the brain, forming masses of either malignant or benign origin. Brain tumors are seen in all ages, including newborns. After middle age, a large number of cancer patients, especially those with cancer, can develop a tumor in the brain due to the spread of the cancer. The resulting mass causes increased intracranial pressure, putting pressure on the brain and causing a number of negative symptoms. Early diagnosis of brain tumors often impacts the patient's life and quality of life. The brain loses its normal structure under the pressure and becomes unable to perform its functions, and the following symptoms are the most common: 1- Headache 2- Epileptic-like fainting spells 3- Partial paralysis in some parts of the body 4- Severe vomiting 5- Loss of some physical abilities 6- Personality disorders Headache: Only patients with brain tumors experience headaches. Our patients report that the pain began in the last few months and has become increasingly severe. Nausea and vomiting: The presence of a headache, especially if it has been present for several days or weeks, is important. However, a prolonged headache and vomiting suggests a migraine. Double vision and blurred vision: Double vision, blurred vision, and decreased vision, with or without a headache, are the first signs of a brain tumor. Weakness, clumsiness, and imbalance in the arms and legs: Recent numbness on the right or left side of the body, weakness, numbness, and clumsiness in the hands may be observed. A "drunken gait" and "unsteadiness" while walking may be symptoms of a cerebellar tumor. Speech disturbances: Inability to speak, difficulty understanding, mispronouncing words, or drunken speech may also be the first signs of a brain tumor. Epilepsy: Involuntary spasms with or without loss of consciousness, and panic attacks, along with feelings of uneasiness, can be a form of epilepsy. These types of seizures, especially those occurring after the age of 20, should be investigated and considered a brain tumor until proven otherwise. Brain tumors can be broadly categorized into two categories: Brain tumors are generally classified as primary or secondary. These tumors (usually) begin elsewhere in the body and metastasize to the brain, and those that develop in the brain. Brain cancers, which are more common in people under 9 and over 55, are more common in Caucasians and males. 1- Benign tumors: They have a slow reproductive rate. They can also be easily separated from brain tissue and can be removed entirely or nearly entirely. Therefore, postoperative outcomes are very good. However, even if the tumor is benign, if it is located in vital, sensitive areas of the brain, the results are unfortunately not satisfactory. 2- Malignant tumors: They grow very quickly and have a mud-like consistency. Therefore, they cannot be completely removed surgically. They grow back within a certain period of time after surgery and continue to press on the brain. Malignant tumors can also be classified according to their reproductive rate. While some tumors offer a survival rate of 5-6 years after surgery, others regenerate within 5-6 months, causing the patient's death. The treatment of brain tumors is surgical. Whether benign or malignant, all tumors are treated surgically. However, in some cases, surgery may not be possible. If the tumor is located in sensitive, vital areas of the brain, the tumor may be left in place, as touching these areas is life-threatening. In this case, only radiation therapy and medication (chemotherapy) can be used. Tumors originating in other parts of the body can spread to the brain. This is called metastasis. Lung cancers, in particular, can spread to the brain and are considered malignant tumors. Even with surgery, the results are often disappointing. In some cases, if there are only a few focal areas of spread, surgery may not even be necessary. The patient is subjected to chemotherapy and radiation therapy. Classification of Brain Tumors: Pituitary Adenomas: Pituitary adenomas are divided into two main groups: hormone-secreting and non-hormone-secreting. Hormone-secreting adenomas generally cause symptoms based on the hormones they secrete. Non-hormone-secreting adenomas, on the other hand, remain asymptomatic for a long time. However, they can cause vision problems by pressing on the optic nerve (the nerve responsible for vision). Hormonal disorders, menstrual irregularities or absence of menstrual periods, breast milk production, obesity, rapid height growth, and growth in the hands, feet, and jaw are all symptoms of hormonal imbalances, and a doctor should be consulted. If the tumor grows significantly, it increases intracranial pressure and causes general symptoms such as headache, nausea, and vomiting. Meningeal Tumors: Meningiomas generally grow, causing increased intracranial pressure and headache, nausea, and vomiting. Epileptic seizures may also occur. These tumors also cause symptoms depending on their location. Those located near the optic nerve (optic nerve) cause vision problems, while those near the brain region responsible for movement can cause strokes. Therefore, necessary tests should be performed for any brain function abnormalities. Metastatic Tumors: Metastatic tumors are tumors that occur when tumors from other parts of the body spread to the brain tissue. These tumors cause symptoms by increasing intracranial pressure and/or causing nervous system damage, depending on their location. These types of spasms can often be the first sign of the tumors. These tumors cause extensive edema that can be visualized radiologically. Pontocerebellar Tumors: These tumors are located in a specific area of the brain tissue. Auditory nerve tumors (acoustic neuromas) are common. Meningiomas (brain meningeal tumors) and epidermoid tumors are also encountered. In addition to the general symptoms of brain tumors, tumors in this area also cause hearing and balance disorders. When these tumors are detected in small sizes, hearing can be preserved. If the tumor is very large, hearing cannot be preserved and the facial nerve may also be affected. Glial Tumors: These tumors are generally malignant and grow within the brain tissue. Their symptoms are general. Again, symptoms depend on their location. Epilepsy (epileptic seizures) may occur as the first symptom in some patients. ø; RELATED DISEASES: Lumbar Spondylolisthesis, Hydrocephalus, Spinal Cord Tumors

